
 |
Lassa Fever Virus |


Lassa infection is an individual from the Old World Arenaviruses, and, all things considered, is endemic in Western Africa. Nonetheless, the full degree of Lassa's endemicity is obscure because of poor mean of contact and correspondence with the country towns where Lassa is most likely seen, an element that anticipates both reporting and treatment of contamination. A few specialists assess the quantity of instances of Lassa contamination at 100,000-300,000, however the number that are accounted for and treated in doctor's facilities is essentially lower. The infection was initially detached in 1969 from a medical caretaker in a Nigerian mission healing facility. No less than two instances of Lassa fever have happened in the United States, the first in Chicago, the second in New Jersey. Both people who had as of late been going in endemic regions of Africa, one in Nigeria, the other in Liberia, and succumbed to the fever in the wake of coming back to the United States. A few occurrences of disease in the lab have happened with Lassa infection, as on account of surely understood virologist Dr. Jordi Casals, who got to be contaminated with the infection in the wake of concentrating on tests from the first Nigerian case.

Transmission:
Lassa virus is typically spread through aerosolized virus particles, via either infected rodents (Mastomys natalensis) or close contact with infected individuals. Additionally, contact with infected bodily fluids, including blood, urine, and vomit, has been known to spread the virus. Virus particles have been isolated from the semen of infected individuals up to six weeks following acute symptoms, and transmission via sexual contact has been implicated in several cases of New and Old World arenaviruses.
Incubation:
The incubation period for Lassa virus is between 5 and 21 days, with symptoms typically appearing 10 days after infection.
Diagnosis:
Traditional laboratory tests provide little help in the way of diagnosis. Leukocyte levels and platelet counts are not useful means of diagnosis. Albuminuria is common. AST levels parallel the amount of virus in the blood, which is a useful factor in determining prognosis. The greater the amount of virus in the blood, the more likely the associated disease will be fatal. Chest X-rays may show some abnormalities, such as pleural effusions, but are most commonly normal. Lassa virus is easily isolated from the blood during the febrile stage of the illness, and CF, IFA, and ELISA may all be used for detecting viral antibodies.

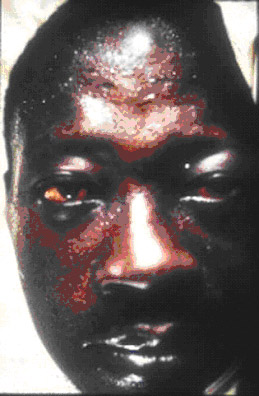
Symptoms:
Fever and malaise generally appear 10 days after infection. As the disease progresses, increased fever and myalgia are typical, accompanied by severe prostration. Gastro-intestinal manifestations, including nausea and vomiting, diarrhea, constipation, and abdominal pain may also appear. In 66% of individuals, sore throat accompanies infection. Cough and retrosternal pain are also common. Hemorrhagic symptoms develop is less than a third of individuals, but are associated with a significant raise in patient mortality. Neurologic phenomena are less common than the aforementioned symptoms, but are nevertheless important. Aseptic meningitis, encephalitis, and global encephalopathy with seizures have all been documented in cases of Lassa virus infection. Intriguingly, deafness is a common feature during late-stage disease or early convalescence, and may be either ephemeral or permanent. While serving as useful diagnostic tool, this manifestation also interrupts individuals’ re-acceptance into their community, and hence plays a role in disease stigmatization. When treated in a hospital setting, mortality rates are between 15% and 20%. However,
Treatment:
Treatment for Lassa fever is largely symptomatic. Management of bleeding and hydration is critical, especially in hemorrhagic cases. Pain management is prescribed through the use of opiates. Due to the permeability of blood vessels, pulmonary edema is a concern, and fluid infusion must therefore be carefully monitored. Ribavirin has been employed principally in Lassa fever patients with poor prognoses, and is usually reserved for patients with an AST value above 150. Though a harsh drug with significant side-effects, ribavirin is the drug of choice in cases of Lassa fever.

ConversionConversion EmoticonEmoticon